Losing a loved one can only be described as deeply saddening and devastating but at least when the cause of that death is unpreventable there is some solace that nothing further could be done. As my family and I are still feeling those effects from the recent loss of my mother I can truly empathise. God only knows what those that lose their children must feel, especially if their lives might have been extended sufficiently to be deemed saved by an organ transplant. After years on dialysis, patients, if they are lucky, may receive a transplant and enjoy a relatively normal, happy life, as my sister’s mother-in-law did until she passed in her 70s, years of freedom she may not have had without that transplant.
You would think then that the proposed change in the law in England to automatically opt-in citizens to the organ donor list would fill me with hope but it doesn't, as there are aspects to organ donation that require deeper inspection and a light shone on them for honest, public debate. As with most things in life, it is not a simple subject no matter how much we would wish it to be so.
What is being proposed?
The Department of Health & Social Care in their document Consultation on introducing ‘opt-out’ consent for organ and tissue donation in England state:
The government considers that it is the right time to revisit the issue of consent and to change the legal default on consent for organ and tissue donation in England. Although 8 out of 10 people say they would want to donate their organs and tissue after their death, most never register to be organ donors. This change would mean the system better reflects the position of the majority of people who would be happy to donate their organs and tissue when they die. It will also respect the decisions of those who do not wish to be organ and tissue donors.
Specifically, they are consulting on the following:
- Proposals to make it easier for people to register their decision on organ and tissue donation. This is to ensure decisions people make about organ donation are honoured after their death.
- Proposals to change the law so that people would be considered willing to be an organ donor unless they decide to opt-out.
- How family members should be involved in confirming decisions in future.
- Proposals for changes, exemptions and safeguards for certain groups of people under the new system.
The document continues:
The core change proposed by the government is on the default legal position. Subject to certain exclusions, described later in this consultation, a person will be considered to have consented to organ and tissue donation after death unless they opt-out.
Let us be clear: the government is intending to change the law so that in England you have consented to donate your organs upon “death” unless you specifically declare that you do not want that to happen by filling out a form to opt-out. Wales already operates a similar system, with Scotland soon to follow and because of an increasing need for organs in England, the government feels that we are also long overdue for that change.
As mentioned in the government’s proposal, it has been widely reported that 50,000 people are alive thanks to organ donation, in addition we have what most would consider a healthy number of potential donors equating to 36% of the UK population, an increase of 6% over a 5 year period. But organ transplants over the same period have increased by 20% with 2016/17 seeing 4,753 procedures performed.
These problems with organ donation were highlighted:
... there is still a shortage of organ donors.
There were 457 people who died last year while on the active transplant waiting list, which means they were ready to receive a donor organ but did not get one in time.
A further 875 people were removed from the list - in most cases because they became too ill to undergo transplant surgery.
There are currently 6,389 people on the active transplant list.
Around 3,000 more people need a donor but are currently suspended from the list.
Reasons for this can include being temporarily too ill to undergo a transplant or because they are abroad.
So what’s the problem with the government’s proposal? Surely, it’s a simple case of 1+1 = 2: people feel it’s a good idea to donate organs, we need more donors so make it an opt-out system. The main focus here though is the change in consent and in that lies the problem.
Informed consent
Informed consent is an area I understand well, as it is the first question posed by medical litigation lawyers to me as an expert witness regarding a negligence action against a healthcare worker (HCW): did the defendant obtain informed consent before performing xyz procedure?
The law regarding informed consent changed with the Montgomery ruling in 2015 in the UK and is important to mention and important for you to understand.
The new ruling was summarised:
Doctors must now ensure that patients are aware of any “material risks” involved in a proposed treatment, and of reasonable alternatives, following the judgment in the case Montgomery v Lanarkshire Health Board.
The British Medical Journal explained it, thus:
The new legal judgement recognises this individual approach to warning patients about risk. Rather than taking into account the percentage possibility of a risk arising, doctors need to bear in mind the significance of a given risk for that particular patient, and the nature of the risk, such as the effect it would have on the patient's life if it were to occur.
In short: HCWs are required by law to not hide any potential risks from a procedure from the patient. It may come as a shock but prior to the Montgomery ruling HCWs did not routinely tell patients of all potential risks. Why is that important now; why should I specifically mention that in relation to the proposed changes in organ donor law?
Well, the obvious answer is that the proposed law is a change to our consenting to organ donation but that’s not the only worry. The real question here is are you being properly informed of all potential risks regarding organ donation in order that you can give informed consent? And that brings us to the subject of death or more specifically, when are you truly dead?
When are you truly dead?
As I was writing this article in between patients it gave me a good opportunity to ask them about their views on organ donation. All pretty much felt it was a good idea and wanted to help the NHS. For those that were already registered as donors, when I questioned them further under what circumstances should their organs be taken they were all clear: when I am dead. My response to that shocked all of them, I stated: organs have to removed still functional and as close to living as possible; no one wants dead organs from a dead body.
Fresh organs are good; dead ones are bad. That of course is a problem to those in the medical profession that want to remove organs as fresh as possible; how can they justify that? The solution to that problem came partly from advanced procedures to “artificially” maintain a breathing body once pronounced “dead”. The other part to the problem was solved by defining a new criterion of death – brain death.
All is not straight forward though and some are suspicious of the alternative definition of death – brain death. Dr Byrne explains in a recorded interview how the criteria for brain death has undergone multiple iterations over many years, each one lowering the bar, in his opinion, to facilitate the removal of organs. He argues that brain death is not true death and that the patient even when confirmed at the stage of brain death can be aware of surgical procedures and pain but unable to communicate to stop it. Dr Byrne is a Catholic doctor and approaches this subject with a religious background and therefore some may criticise his opinion as biased; others, may not. However, his opinions are shocking especially when you consider that he is one of the founders of neonatology (that deals with the diseases and care of newborn infants), a significant achievement by Dr Byrne that argues, at the very least, that he be taken seriously.
He points out that the criteria for brain death originally called the Harvard criteria in 1968 did not follow the normal scientific method, at best it was an educated guess. Dr Byrne specifically criticises the apnoea test used by doctors to help decide whether a patient is dead or not. The test involves removing the patient from oxygen and seeing if they spontaneously breathe by themselves, the test lasts 10 mins. He contends that doing that will almost assure that the patient will be harmed. Research in that area does support that procedure and suggests that appropriate precautions be made to ensure the safety of the patient but common sense and the literature suggests there are inherent dangers:
Complications associated with apnea testing include hypoxemia, hypotension, acidosis, hypercapnia, increased intracranial pressure, pulmonary hypertension, and cardiac arrhythmias (Table 3).14 –20 Cases of cardiac arrest and pneumothorax have also been reported.21 Certain complications can be considered inherent, due to the nature of the test itself…
Hypoxemia during apnea testing further increases the potential risk for cardiac dysrhythmias and hypotension. Appropriate precautionary steps, such as pre-oxygenation with 100% oxygen, are essential to prevent hypoxia during apnea testing, should be used, and have been shown to be effective.14,17
Dr Byrne is not alone in criticising brain death, other experts such as Dr Karakatsanis argues that brain death needs to be re-evaluated. His stated objectives for his research paper were:
To evaluate whether current clinical criteria and confirmatory tests for the diagnosis of ‘brain death’ satisfy the requirements for the irreversible cessation of all functions of the entire brain including the brainstem.
His research was deeply concerning:
We present four arguments to support the view that patients who meet the current operational criteria of ‘brain death’ do not necessarily have the irreversible loss of all brain (or brainstem) functions. First, many clinically ‘brain-dead’ patients maintain residual vegetative functions that are mediated or coordinated by the brain or the brainstem. Second, it is impossible to test for any cerebral function by clinical bedside exam, because the tracts of passage to and from the cerebrum through the brainstem are destroyed or nonfunctional. Furthermore, since there are limitations of clinical assessment of internal awareness in patients who otherwise lack the motor function to show their awareness, the diagnosis of ‘brain death’ is based on an unproved hypothesis. Third, many patients maintain several stereotyped movements (the so-called complex spinal cord responses and automatisms) which may originate in the brainstem. Fourth, not one of the current confirmatory tests has the necessary positive predictive value for the reliable pronouncement of human death. [My emphasis].
Dr Karakatsanis concludes:
According to the above arguments, the assumption that all functions of the entire brain (or those of the brainstem) in ‘brain-dead’ patients have ceased, is invalidated. Reconsideration of the current concept of ‘brain death’ is perhaps inevitable.
Couple that research with what we have been discovering about human consciousness and death, especially near death experiences (NDE) and evidence of life after death then the idea that you would remove someone’s organs based on brain death or circulatory death (discussed later) becomes more disturbing:
Recollections in relation to death, so-called out-of-body experiences (OBEs) or near-death experiences (NDEs), are an often spoken about phenomenon which have frequently been considered hallucinatory or illusory in nature; however, objective studies on these experiences are limited.
In 2008, a large-scale study involving 2060 patients from 15 hospitals in the United Kingdom, United States and Austria was launched. The AWARE (AWAreness during REsuscitation) study examined the broad range of mental experiences in relation to death. Researchers also tested the validity of conscious experiences using objective markers for the first time in a large study to determine whether claims of awareness compatible with out-of-body experiences correspond with real or hallucinatory events.
They concluded:
- The themes relating to the experience of death appear far broader than what has been understood so far, or what has been described as so called near-death experiences.
- In some cases of cardiac arrest, memories of visual awareness compatible with so called out-of-body experiences may correspond with actual events.
- A higher proportion of people may have vivid death experiences, but do not recall them due to the effects of brain injury or sedative drugs on memory circuits.
- Widely used yet scientifically imprecise terms such as near-death and out-of-body experiences may not be sufficient to describe the actual experience of death. Future studies should focus on cardiac arrest, which is biologically synonymous with death, rather than ill-defined medical states sometimes referred to as ‘near-death’.
- The recalled experience surrounding death merits a genuine investigation without prejudice.
Dr Parnia’s research suggests that death is not what we originally thought:
Contrary to perception, death is not a specific moment but a potentially reversible process that occurs after any severe illness or accident causes the heart, lungs and brain to cease functioning…
…consciousness and awareness appeared to occur during a three-minute period when there was no heartbeat. This is paradoxical, since the brain typically ceases functioning within 20-30 seconds of the heart stopping and doesn’t resume again until the heart has been restarted. Furthermore, the detailed recollections of visual awareness in this case were consistent with verified events. [My emphasis].
Even though traditional wisdom would state that the brain had stopped functioning and therefore consciousness and awareness could not continue, they had demonstrated in the research that the brain had stopped functioning and the patient was conscious and aware.
Well, at least an anaesthetic is administered to the organ donor prior to removal of their organs, right? Just in case?
That’s a question that was posed during an exchange on a nurses forum:
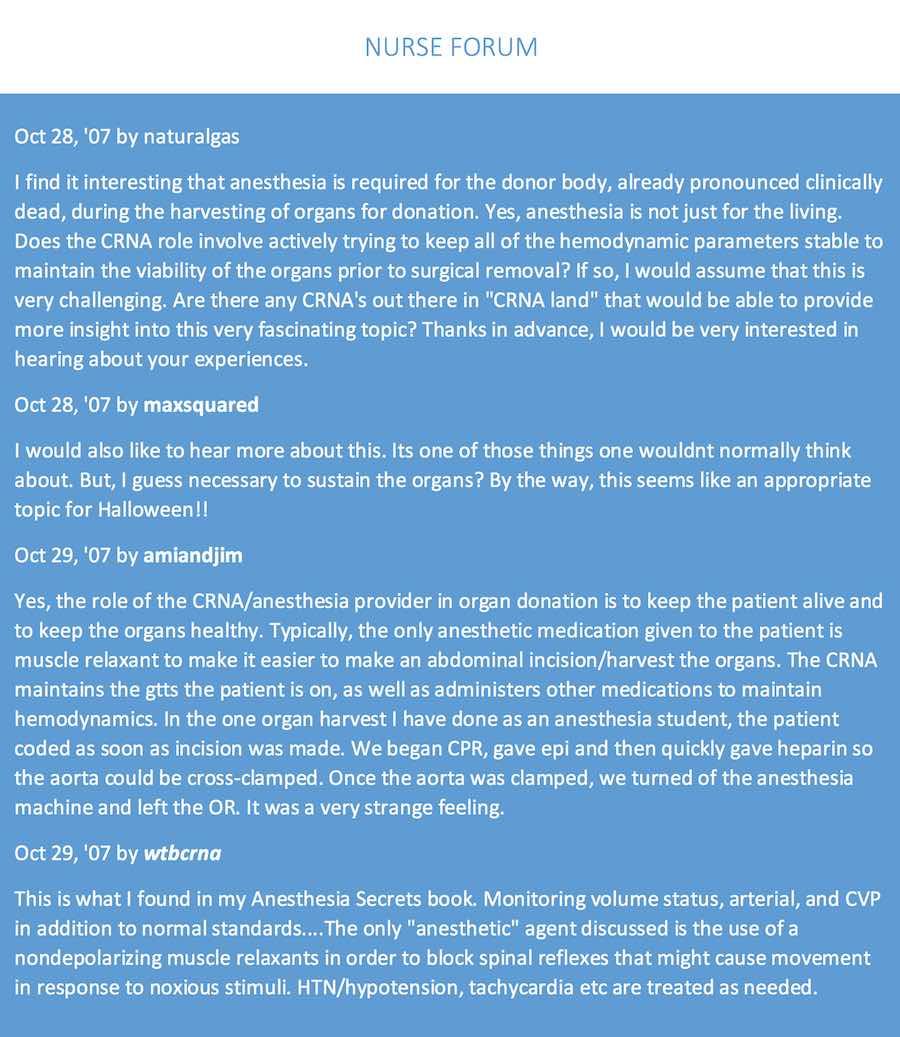
In case you missed that: no anaesthetic is given; only drugs to maintain the body and one other – a paralysing drug called a non-depolarising blocking agent. Yes – a drug to paralyse you while they take the organs with no anaesthetic.
Regarding those non-depolarising agents:
Patients are still aware of pain even after full conduction block has occurred; hence, general anaesthetics and/or analgesics must also be given to prevent anaesthesia awareness.
Unfortunately, neither anaesthetics nor analgesics are given. In the exchange between the nurses it is mentioned that the non-depolarising blocking agent is given to improve the surgical field aka make it easier to cut through parts of the body but Dr Byrne offered some chilling anecdotal evidence from colleagues involved in those procedures prior to the use of non-depolarising blocking agents that gives a different take.
[The patient] was not even given anaesthetic when they took the organs but they were paralysed so that they didn’t move and cause any discomfort to the people in the operating room who might see them, as one transplant surgeon said, ‘as I made the incision down the middle of the chest to take the organs the man threw both arms out’. And of course that was several years ago and it doesn’t happen anymore because the paralysing agent does not allow that to happen.
What may also be disturbing to you is that Lacrimation or crying is common among donors as their organs are removed:
Also, during the early stages of organ removal lacrimation is a common phenomenon.45 According to Gray’s Anatomy, ‘Preganglionic fibres probably arise from a special lacrimatory nucleus in the lower pons…These fibres synapse in the pterygopalatine ganglion which they leave in one of its branches…, to reach the lacrimal nerve. Thus they supply secromotor fibres to the gland’.46
Therefore, lacrimation in ‘brain-dead’ patients is an evidence that the lacrimatory nucleus in the brain stem is viable.
Disturbing, and proof that the donor is not brain dead.
What is the UK’s position on diagnosing death? Transplantation from deceased donors after circulatory death published by the British Transplantation Society explains:
Prior to the introduction of guidance defining the concept of brain death in the 1970s, all organs for transplantation were donated after circulatory death (DCD). Following the introduction of brain stem death testing, the majority of organs for transplantation were donated after brain death (DBD) or, increasingly, from living donors.
And although research and guidelines exist:
…there remains no statutory definition of death in the UK and the working definition ‘the irreversible loss of the capacity for consciousness combined with irreversible loss of the capacity to breathe’ put forward by the Department of Health seems to have been adopted as the pragmatic approach.
It details:
Neurological and circulatory functions are inextricably linked. Death – i.e. the loss of capacity for consciousness and all brain stem function – most commonly occurs following the loss of circulatory function from which a patient should not be or cannot be resuscitated.
And states that circulatory death can be
Confirmed through absence of consciousness, respiration and other brain stem functions after the agreed period of observation, which should be a minimum of seven minutes.
NHS Blood and Transplant define the different death criteria:
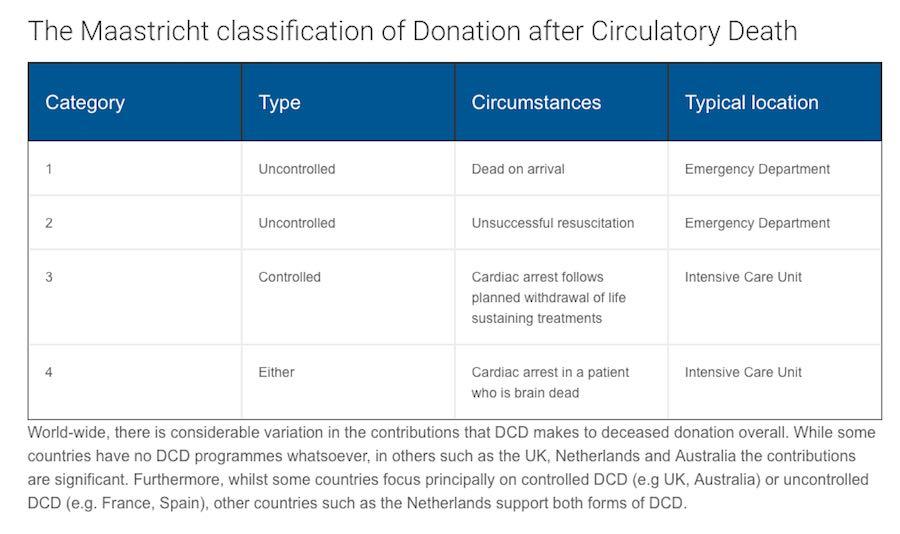
Donation after Circulatory Death (DCD), previously referred to as donation after cardiac death or non-heartbeating organ donation, refers to the retrieval of organs for the purpose of transplantation from patients whose death is diagnosed and confirmed using cardio-respiratory criteria.
There are two principal types of DCD, controlled and uncontrolled. Uncontrolled DCD refers to organ retrieval after a cardiac arrest that is unexpected and from which the patient cannot or should not be resuscitated. In contrast, controlled DCD takes place after death which follows the planned withdrawal of life-sustaining treatments that have been considered to be of no overall benefit to a critically ill patient on ICU or in the Emergency Department. The clinical circumstances in which DCD can occur are described by the Maastricht classification.
is possible from patients whose death has been confirmed using neurological criteria (also known as brain-stem death or brain death).
Neurological criteria for the diagnosis and confirmation of death applies in circumstances where brain injury is suspected to have caused irreversible loss of the capacity for consciousness and irreversible loss of the capacity for respiration before terminal apnoea has resulted in hypoxic cardiac arrest and circulatory standstill. This diagnosis is only possible in patients who are on mechanical ventilation
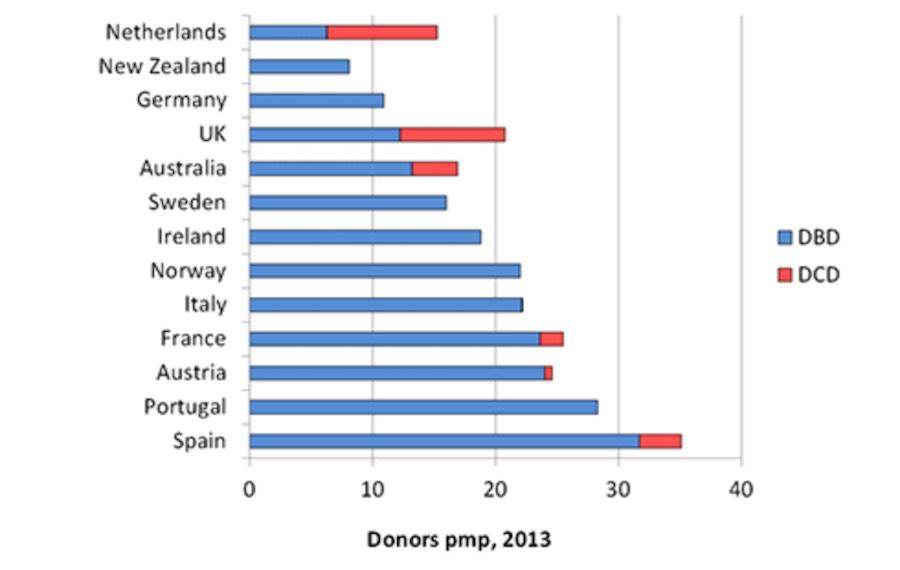
The data clearly show that the largest percentage of organs come from brain death donors compared to circulatory death donors. That fact becomes important due to the evidence demonstrating conscious awareness in those believed to be brain dead. The UK guidelines vary but waiting 5 – 7 minutes after circulatory death along with other testing to confirm “death” is more reassuring compared to other countries that wait seconds but nonetheless as our knowledge of conscious awareness and death develops, can we be sure that that is sufficient time for the donor to truly die?
The above information is disturbing but equally or more disturbing is the knowledge that there are those that would gladly profit from organ donors.
Profit, black market & corruption
There were 525,048 deaths in the England & Wales in 2016 and an average body is valued up to $5,000,000 or £3,700,485 for its organs. With some estimates exceeding $12,000,000 or £8,712,096 when aftercare is factored in. With demand for organs growing both nationally and internationally, even if only half of those deaths were monetised at just 10% of the potential value of each body at £3,700,485 that equates to a staggering 97 billion, 146 million, 612 thousand, 414 pounds (£97,146, 612, 414) generated per year.
No one is suggesting that the supply of human organs obtained from those that have died (that are not conscious and aware and do not feel pain) in order to extend the lives of desperately ill patients is nothing less than a generous act of compassion. But if organs are to be removed for profit without really knowing if the donor will suffer to give up those organs is, of course, unthinkable and more akin to human factory farming and to be condemned in the strongest possible terms.
But could the unthinkable happen and the NHS be seen as cash cow for organs? Could financial pressures and targets driven by managers and hospital policy bias decisions over whether to extend life or remove precious organs? Is the proposed law a cynical move to increase profitability, making the NHS a much more attractive proposition for private investment and takeover? I dearly hope not and one hopes that the proposed change in English law to automatically opt-in its citizens for organ donation is purely altruistic and reflects the good will of the NHS staff and UK citizens but with a growing market for organs worldwide and a rapidly approaching privatised NHS, questions have to be asked: will this change to the law really serve the people of this country? And is there potential for abuse as a result of that change?
Dr Dale Archer shines a light on the darkness that is organ harvesting in his article Body Snatchers: Organ Harvesting For Profit:
Recently in China, a missing 6-year-old boy was found alone in a field, crying. Upon closer inspection, both eyes had been removed, presumably for the corneas.
In 2012, a young African girl was kidnapped and brought to the UK for the sole purpose of harvesting her organs. She was one of the lucky ones—rescued before she went under the knife. Authorities feel this is just the tip of the iceberg.
…Kendrick Johnson, a Georgia teen, died at school January 2013. The local sheriff quickly determined the death was a freak accident, that he suffocated after getting stuck in a rolled up mat in the school gym. Johnson's parents however, could not—would not—accept that. Six months after his death, they obtained a court order to have the body exhumed for an independent autopsy.
The pathologist was stunned when he found the corpse stuffed with newspaper. The brain, heart, lungs and liver were missing. He also discovered Johnson's death was due to blunt force trauma to the right side of his neck. The FBI is now involved in this disturbing case with potentially shattering reverberations.
That was just a small sample of cases and outside the medical profession but could the profession be corrupted?
Sadly, corruption is endemic in the medical profession as has been reported in the medical literature:
A linked editorial made it clear that India was not alone in having a deeply embedded culture in medicine of tolerance to and even promotion of corruption (doi:10.1136/bmj.g3169). If anyone doubted this, recent news from the United States suggested that healthcare corruption was equally endemic there. On top of evidence that the US loses billions of dollars each year to medical embezzlement (http://econ.st/1BuAiFW), high profile cases are now making clear the mechanisms and the human cost. Six doctors in Chicago are currently being prosecuted for allegedly taking kickbacks. Their alleged crimes includes referring patients to hospital who didn’t need admission and performing unnecessary but lucrative tracheotomies, leading to avoidable deaths (doi:10.1136/bmj.h22).
Nor, sadly, is the United Kingdom immune. A BMJ investigation published this week reports clear evidence of UK doctors receiving covert financial inducements to refer patients to private hospital groups. Some London based doctors have benefited by tens, sometimes hundreds, of thousands of pounds (doi:10.1136/bmj.h396).
A 2017 study by the european commission as reported in Global Compliance News also demonstrated widespread corruption:
The 2017 Study concluded that the healthcare sector is one of the areas that is particularly vulnerable to corruption. The results of the study relevant for companies in the healthcare sector were that
1. bribery in medical service delivery remains one of the main challenges, especially in many Eastern and Southern European Member States.
2. transparent procedures are key in addressing corruption in procurement processes.
3. attempts to address improper marketing increase at both EU and national level.
There were six typologies of corruption identified:
1. bribery in medical service delivery;
2. procurement corruption;
3. improper marketing relations;
4. misuse of (high) level positions;
5. undue reimbursement claims;
6. fraud and embezzlement of medicines and medical devices.
A German doctor was charged with manslaughter and falsifying hospital data in order to facilitate organ transplants for his patients:
In a case expected to shed light on a major Europe-wide organ donation scandal, a 46-year-old doctor went on trial in Germany charged with 11 counts of attempted manslaughter and systematically falsifying hospital data to procure speedy transplants for his patients.
A 2015 Mercury News article on organ harvesting clearly demonstrates, at one extreme, the danger of unrestrained, unaccountable government and organ transplanting as it details a report entitled Bloody Harvest/The Slaughter: An Update. It was authored by former Canadian Secretary of State David Kilgour, investigative journalist Ethan Gutmann and distinguished human rights lawyer David Matas:
It gives a chilling figure of up to 1.5 million prisoners of conscience being killed for their organs by the Chinese regime. Prisoners of conscience primarily are practitioners of Falun Gong who were locked up for their beliefs. It was just months after the persecution of Falun Gong began in July 1999 when organ transplant volume in China increased exponentially…
'We provide considerable evidence of an industrial-scale, state-directed organ transplantation system, controlled through national policies and funding, and implicating both the military and civilian health care systems,' Kilgour said to the European Parliament on June 30. 'The kidneys, livers and hearts are often sold on demand to overseas patients, who can afford them. That is, the prisoners of conscience are tissue typed and then killed once a matching recipient is found for their organs,' according to the website of the International Coalition to End Organ Pillaging in China.
The Alliance for Human Research Protection in their article entitled US Organ Harvesting in “Not Yet Dead” patients is nothing short of shocking as it lays out just how the pressure to obtain organs can lead to practises that are only a few steps removed from those alleged to be taking place in China:
The Washington Post reports that 'a new trend' in organic harvesting is underway within minutes of cardiac arrest. This government sanctioned program euphemistically called, 'donation after cardiac death' (DCD) accelerates the organ 'donation' process.
Some doctors and bioethicists, however, say the practice raises the disturbing specter of transplant surgeons preying on dying patients for their organs, possibly pressuring doctors and families to discontinue treatment, adversely affecting donors’ care in their final days and even hastening their deaths.
'The person is not dead yet,' said Jerry A. Menikoff, an associate professor of law, ethics and medicine at the University of Kansas. 'They are going to be dead, but we should be honest and say that we’re starting to remove the organs a few minutes before they meet the legal definition of death.'
The Post reports: 'When surgeons resurrected what was then called “non-beating heart' donation in the 1990s, critics called it ghoulish and said it raised a host of ethical questions. Some called it tantamount to murder.'
The practise doesn’t spare children either as the article informs us how a Denver Children’s Hospital waits just 75 seconds before taking the hearts of infants.
Others have also raised concerns that border on eugenics:
There are far too many mysterious shootings taking place in this country [USA], especially so-called clean shootings, in which the only fatal wound is a shot to the head, leaving vital organs unaffected and eligible for harvesting…
African Americans are the targets of a policy very dangerous for us but extremely lucrative financially for the people who make the policy but care little about the consequences of the policy being implemented.
Of course, organ donation and harvesting is an international concern not limited to our discussion here of “peaceful” civil society but also is hugely implicated in war torn countries with official recognition of harvesting in Kosovo during the 1998-99 war and more recently Syria. Although, there is debate about just who is doing what to whom, as propaganda abounds across the web.
It is a slippery and treacherous slope we walk as we tamper with consent law and naively stumble from altruistic medicine to a target driven, profit generating, healthcare business. As we have seen, evidence from across the EU, USA & China should be a red flag to anyone that believes otherwise.
In addition, as we move from a human focused society to a post-human/transhuman one in the Fourth Industrial Revolution, where the respect and primacy of the human is diminished, what will constrain those that feel they would benefit from your organs and have the means to obtain them?
Clues, like faint echoes from the literature of the past and more recent publications, reverberate as warnings to those that have eyes and ears to notice where society has been and may become again. As we conclude this article on organ donation let us not forget just what the medical profession is capable of. From the Annals of Internal Medicine: 15 February 2000:
In the United States and Germany before World War II, physicians participated in state-authorized eugenic sterilization programs in an attempt to prevent persons deemed to possess undesirable heritable characteristics from propagating. A comparison of U.S. and German histories reveals similarities that argue against easy dismissal of a Nazi analogy. On the basis of a review of editorials in New England Journal of Medicine and Journal of the American Medical Association from 1930 to 1945 it is difficult to accept the suggestion that the alliance between the medical profession and the eugenics movement in the United States was short-lived.
Thankfully, that practise was overturned as sane men and women prevailed over those so deranged as to experiment on those they felt superior to, and who were too weak or without influence enough to prevent them from doing so.
From the Institute of Ethics and Emerging Technologies April 19th 2017, a UK professor writes in A Modest Proposal for Suicide as a Facilitator of Transhumanism:
Perhaps the most potent argument against suicide in modern secular societies is that it constitutes wastage of the agent’s own life…However, the force of this argument could be mitigated if the suicide occurred in the context of experimentation, including self-experimentation, with very risky treatments that aim to extend the human condition. Suicides in these cases could be quite informative and hence significantly advance the prospects of the rest of humanity. The suicide agent’s life would most certainly not have been in vain.
He continues:
My modest proposal is that the taboos on suicide be lifted such that potential experimental subjects who are told that their chances of survival are very uncertain may nevertheless agree to participate with limited liability borne by the institution conducting the research…
even including a level [of risk] that implies a much higher likelihood of death than most people would tolerate. Such people have the makings of becoming the true of heroes of the transhumanist movement.
Suggesting experimenting on people contemplating suicide from a UK professor is significantly disturbing. We must remember that everything is context and what seems impossible today may not be so in the near future (just like the past), especially if human dignity is diminished to the point that our compassion and love for our fellow humans is extinguished so that we see them as body parts to be experimented on and profited from. Then nothing is sacred, not even unborn babies.
What we must consider is how the erosion of consent may play out. A perfect example is vaccination where initially in the US citizens were asked to consent for vaccination; then some vaccines were made compulsory but you could opt-out; then gradually the ability to opt-out was removed and more vaccines were made compulsory. Will organ donation follow suit? Will there be a time when you cannot opt-out?
If the evidence we have discussed that brain death is not true death and donors may be aware and conscious, and with some procedures to remove organs taking over an hour and the donor possibly being aware throughout some of that process, it simply doesn’t bear thinking about. Some doctors have stated that certain transplant procedures are akin to murder but with murder at least you can die, and hopefully quickly, instead of intentionally being kept alive by HCWs prior to organ removal in one instance or after you have “died” in another, with both scenarios waiting mere minutes before organs are removed with no anaeshetic, all under the pretense that the donor is truly dead and not conscious and aware. However, we know that may not always be the case and the donor may endure unspeakable suffering.
Everything starts from the first step; in the case of organ donation, let us not repeat the mistakes of the past, and make sure that our steps are in the right direction.
In closing
Any law that assumes consent in such an important area, before being passed, must first prove beyond any reasonable doubt that we can ascertain that the organ donors are truly dead and that no abuse or profiteering will be tolerated from the use of donated organs either in the NHS as it stands now or sometime in the future when undoubtedly it will be privatised. Currently, it would seem that the evidence regarding brain death suggests that the government cannot prove the case for organ donation absent inflicting harm and cruel suffering on the donor. In circulatory death, the provision of waiting 5 - 7 minutes along with other testing may offer a degree of confidence but as new research comes to light even that criteria may be challenged as not definitively proving death. It is also doubtful, especially if financial interest enters the equation, that increasing pressure to remove organs could be prevented, putting patients at risk and destroying confidence in the system of organ donation.
Whether you agree or not with the definition and method of proving death; and whether or not you are persuaded that there is significant evidence that some donors may not in fact be dead and may still experience pain upon dissection for removal of organs; and whether or not you believe that financial interests may impact the decision to remove organs or preserve life, the decision to donate your organs is yours and yours alone. And that decision must include all available information regarding organ donation, it is not for the government or any HCW to make that decision for you and it is not up to them to withhold information that may affect your decision. In fact, according to the Montgomery ruling it is unlawful to do so.
Anyway, at least now you have been informed … so choose wisely what you consent to.
