Fact checkers and official media talking heads accuse anyone who suggests that "COVID is a hoax" of being COVID deniers, conspiracy theorists and of exhibiting a callous disregard for lives allegedly lost to the disease.
When Piers Corbyn addressed a crowd in Liverpool in October last year, the Liverpool Echo reported his words as follows:
This Covid-19 virus is a hoax. There may have been something around in China, was it the same thing, was it a bio-weapon, who knows. But it was used to unleash the most monstrous power-grab the world has ever seen.
He was questioning the official narrative we have been given about COVID-19, openly declaring his doubt about both its origin and the nature of the disease. However, the thrust of his argument was political. The "hoax" Piers Corbyn was referring to was the exploitation of COVID-19 to justify the seizure and centralisation of authoritarian political power.
In response to this allegation, the Echo reported:
Mr Corbyn's speech came two days after the brother of Liverpool Mayor Joe Anderson died following a battle with severe Covid-19.
Yesterday the ECHO also reported the death of Liverpool music legend Hambi Haralambous, who posted a warning to his Facebook friends at the end of September.
The post included a photo of him in his hospital bed wearing a bubble-like ventilation helmet, connected to an oxygen supply and an array of medical equipment, alongside the simple warning: "To all my Facebook friends who think Covid is a hoax. Think again."
The insinuation is obvious: in suggesting that COVID-19 was a "hoax", Piers Corbyn, and all those who agreed with him, were disrespecting the memory of those who have died "with" COVID. This argument deploys a number of logical fallacies, the two most obvious being appeal to emotion and the strawman.
Instead of a rational argument, mainstream media were relying upon powerful imagery and sorrow. Their intention was to illicit an emotional response in the reader. They then falsely alleged that by questioning COVID-19, Piers Corbyn and the gathered crowd were disrespecting the lives lost. This was an attempt to claim moral superiority.
The use of such propaganda techniques seems to have been deliberate and calculated. They were designed to stop logical consideration of the arguments, increasing the chance that the core allegation of a political power grab would be discarded by the reader as unthinkable, obscene or a disgusting slur; to create a false belief based upon emotion rather than rationalism.
The pejorative loading of "hoax" presents a significant problem for critics who are trying to reach a wider audience. Anyone who questions lockdowns and the statistical or scientific evidence, supposedly informing policy, can then be accused of COVID denial. This is another loaded term which exploits the appeal to emotion fallacy. The allusion to Holocaust denial is obvious.
Appeal to Authority
Collectively, this litany of logical fallacies, incessantly deployed by mainstream media, culminate in the central falsehood of appeal to authority. We must not question what government and global health authorities tell us about COVID-19. We must trust them because the authorities have a special and profound grasp of reality: one we must all appreciate. Questioning authority has become heretical.
Despite appearances, the science surrounding COVID-19 is not settled and the medical profession are not all of one mind. The government have selected a small band of scientific advisors and have ignored every other strand of scientific and medical opinion. Their grasp of the truth is no better than anyone else’s.
There are valid reasons to ask if COVID-19 exists and we will explore them in this article. We do so because neither certainty nor consensus is a core principle of science and reason.
Has SARS-Cov-2 Been Isolated?
There has been a considerable amount of discussion about the isolation, or not, of SARS-CoV-2. The argument proposed by critics is that unless something can be separated from other genetic material, in its purified form, it cannot be said to have been isolated.
If it hasn't been isolated for study how can its independent existence be established? If the existence of SARS-CoV-2 can’t be established, then where does that leave COVID-19?
People have been at pains to point out that Koch's Postulates have not been met for SARS-CoV-2. These describe the conditions that must be met in order for a causative relationship between a microorganism and a disease to be established:
(1) The microorganism must be found in diseased but not healthy individuals;
(2) The microorganism must be cultured from the diseased individual;
(3) Inoculation of a healthy individual with the cultured microorganism must recapitulated the disease;
(4) The microorganism must be re-isolated from the inoculated, diseased individual and matched to the original microorganism.
Robert Koch, alongside Louis Pasteur and Joseph Lister, are considered the founders of germ theory. This describes the concept that disease is caused by invading microorganisms. It is the basis for modern, western allopathic medicine.
Germ Theory views the human body as an uninfected biological system that must be defended against external attack. Should microorganisms (germ - viruses) invade the system, then they need to be destroyed.
Our natural immune system can't always do this, resulting in disease that can sometimes be fatal. Medicine must intervene, either by protecting the system against attack (often using vaccines) or by destroying the invader (drugs, surgery, radiation, chemotherapy etc.)
Robert Koch came to believe that his first condition wasn't valid after he discovered claimed asymptomatic cholera and typhoid. This has led some to suggest that Koch's postulates somehow don't count and that those who ask if COVID-19 exists are idiots for suggesting they should. Laughing heartily at the veneration of 19th century science and exulting in how far we have advanced since then, they fail to offer a better definition of causality themselves.
What is Disease?
We have advanced so far that there isn't even a widely accepted formal definition of disease, let alone what causes it. However from the Encyclopedia Britannica we have:
Disease, any harmful deviation from the normal structural or functional state of an organism, generally associated with certain signs and symptoms and differing in nature from physical injury.
A symptom is some physical or psychological change which can be observed. This may be experienced by the infected person, for example the dry cough associated with COVID-19, or it could be something imperceptible, such as painless tumour growth.
A sign is the potential evidence of something. A positive RT-PCR test is a sign that you are, or have been in the past, infected with SARS-CoV-2. It doesn't mean you have COVID-19. A doctor would need to consider both signs and symptoms to make a diagnosis.
This questions the concept of asymptomatic disease. Modern medicine commonly screens for disease without symptoms; early screening for cancer for example. However, this screening is looking for signs of a potential diseased not necessarily the disease itself, though that may also be present. Concerns have been raised that this results in over-diagnosis with people undergoing high risk treatments for a disease they don't have.
COVID-19 symptoms are hardly unique. The NHS list them as:
- a high temperature
- a new, continuous cough
- a loss or change to your sense of smell or taste
Most people with SARS-Cov-2 have at least one of these symptoms.
Just one of these symptoms, which could be attributable to practically any respiratory illness, bacterial infection, allergy or even air pollution is supposedly sufficient for a doctor to at least suspect COVID-19. When combined with a positive test then, based upon the available evidence, a diagnosis of COVID-19 seems likely.
Perhaps Robert Koch was too hasty to abandon his first postulate. Certainly it is very hard to see how anyone can be said to have a disease based upon signs alone. Yet that is exactly how COVID-19 has been attributed in an unknown number of alleged "cases".
Koch’s Postulates Updated
In 1937, with the new emerging science of virology, Thomas M Rivers offered a new version of Koch's Postulates. Rivers' amended postulates required that the following conditions be met to prove a virus caused a disease:
1. Isolation of virus from diseased host
2. Cultivation of virus in host cells
3. Proof of filterability
4. Produce same disease in host
5. Re-isolation of virus
6. Detection of a specific immune response to virus
This was necessary because a virus could not possibly meet Koch's criteria. Viruses are incapable of replication outside of a host cell or in any neutral medium. Isolation, as suggested by Koch, is therefore not feasible for a virus.
As science progressed, with the DNA revelations of Watson and Crick in 1953, further amendments were made to the proof demonstrating viral causation of a disease. In 1996 Fredricks and Relman published an update of Rivers Postulates for the viral DNA age:
1. A nucleic acid sequence belonging to a putative pathogen should be present in most cases of an infectious disease. Microbial nucleic acids should be found preferentially in those organs or gross anatomic sites known to be diseased, and not in those organs that lack pathology.
2. Fewer, or no, copies of pathogen-associated nucleic acid sequences should occur in hosts or tissues without disease.
3. With resolution of disease, the copy number of pathogen-associated nucleic acid sequences should decrease or become undetectable. With clinical relapse, the opposite should occur.
4. When sequence detection predates disease, or sequence copy number correlates with severity of disease or pathology, the sequence-disease association is more likely to be a causal relationship.
5. The nature of the microorganism inferred from the available sequence should be consistent with the known biological characteristics of that group of organisms.
6. Tissue-sequence correlates should be sought at the cellular level: efforts should be made to demonstrate specific in situ hybridization of microbial sequence to areas of tissue pathology and to visible microorganisms or to areas where microorganisms are presumed to be located.
7. These sequence-based forms of evidence for microbial causation should be reproducible.
Modern science appears to have moved us a long way from the proof of causality suggested by Koch to the far less categorical possibilities offered by Fredricks and Relman. Science rarely deals in certainty and new evidence must be accounted for. This tends to shift it towards greater complexity.
Nonetheless, we shouldn't assume that added uncertainty necessarily moves us closer to the truth. Especially when fundamental concepts, such as causality for a disease, have alternative explanations.
Again, Has SARS-Cov-2 Been Isolated?
It wasn't critics of the COVID-19 narrative who started the debate about claimed "isolation." Following the World Health Organisation's (WHO's) classification of COVID-19 (2019-nCoV renamed COronaVIrus Disease 2019), their laboratory testing guidance said:
The etiologic agent [causation for the disease] responsible for the cluster of pneumonia cases in Wuhan has been identified as a novel betacoronavirus, (in the same family as SARS-CoV and MERS-CoV) via next generation sequencing (NGS) from cultured virus or directly from samples received from several pneumonia patients.
In the WHO's Novel Coronavirus 2019-nCov Situation Report 1, they noted:
The Chinese authorities identified a new type of coronavirus, which was isolated on 7 January 2020……On 12 January 2020, China shared the genetic sequence of the novel coronavirus for countries to use in developing specific diagnostic kits.
The WHO were claiming that the SARS-CoV-2 virus had been isolated and they gave the impression that genetic sequences were identified from the isolated sample. Diagnostic kits were subsequently calibrated to test for this virus and distributed globally. However, the WHO also stated:
Working directly from sequence information, the team developed a series of genetic amplification (PCR) assays used by laboratories.
The Wuhan scientists developed their genetic amplification assays from "sequence information" not from an isolated sample of any virus. The WHO cited their work as proof of isolation. Yet it was the Wuhan research scientists themselves who stated:
The association between 2019-nCoV and the disease has not been verified by animal experiments to fulfil the Koch's postulates to establish a causative relationship between a microorganism and a disease. We do not yet know the transmission routine of this virus among hosts.
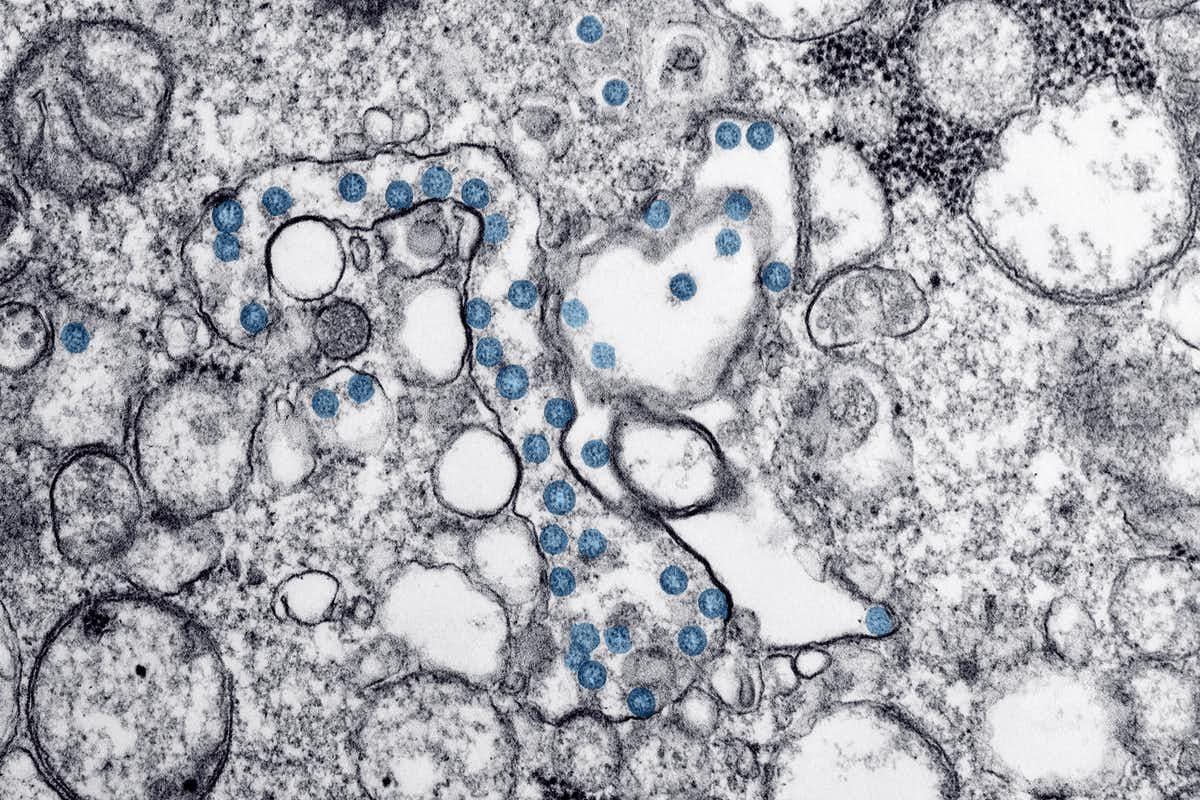
They had pieced the SARS-CoV-2 genome together by matching fragments (nucleotide sequences) with other, previously discovered, genetic sequences. Using de novo assembly, they subsequently employed quantitative PCR (RT-qPCR) to sequence 29,891-base-pair (bp) that collectively shared a 79.6% sequence match to SARS-CoV. As they found more than 29,000 bp the genome was considered complete.
SARS-CoV (SARS-CoV-1) was discovered in 2003 in Hong Kong by scientists who studied 50 patients with severe acute respiratory syndrome (SARS). They took samples from two of these patients and developed thirty cloned cultures in fetal monkey liver cells. Analysis revealed that there was genetic material of "unknown origin" in one of these thirty cloned samples.
The Hong Kong team examined this unknown material and found a 57% match to bovine coronavirus and murine hepatitis virus. They concluded it must be from the Coronaviridae family. The researchers stated:
Primers for detecting the new virus were designed for RT-PCR detection of this human pneumonia-associated coronavirus genome in clinical samples. Of the 44 nasopharyngeal samples available from the 50 SARS patients, 22 had evidence of human pneumonia-associated coronavirus RNA.
While all of the Hong Kong patients were diagnosed with symptoms of SARS only half of them tested positive for the SARS-CoV-1 virus. To date, we don't know why the other half didn't.
With a 57% sequence match to known coronavirus, 43% of the genetic material in SARS-CoV-1 was unaccounted for. The new genome was then registered as GenBank Accession No. AY274119.
The Wuhan Centre for Disease Control and Prevention and the Shanghai Public Health Clinical Centre published the SARS-CoV-2 genome as Genbank Accession No. MN908947.1. It was a 79.6% genetic sequence match to a 57% genetic sequence match of a suspected betacoronavirus found in one of thirty cloned samples taken from two patients in Hong Kong in 2003.
This was the basis for the WHO's claim that SARS-CoV-2 was isolated on 7 January 2020.
Isolation did not mean separation but rather genomic sequencing, and the Wuhan team that conducted the research were the first to point out that Koch's Postulates hadn't been met for SARS-CoV-2, rendering the sneering rejection of related criticisms as unscientific rather absurd.
Drosten to the Rescue
The WHO then used a paper published by Corman Drosten et al as the basis for their RT-qPCR protocol for detection and diagnostics of 2019-nCoV. This defined the RT-PCR tests used the world over to detect SARS-CoV-2 in tested samples. Many scientists consider the Corman Drosten paper to be so poor they have requested its immediate withdrawal from publication.
Among the deluge of criticisms, including an apparent lack of peer review, no use of negative controls and the notable absence of any standard operational procedure, the scientists observed:
The first and major issue is that the novel Coronavirus SARS-CoV-2 … is based on in silico (theoretical) sequences, supplied by a laboratory in China, because at the time neither control material of infectious ("live") or inactivated SARS-CoV-2 nor isolated genomic RNA of the virus was available to the authors. To date no validation has been performed by the authorship based on isolated SARS-CoV-2 viruses or full length RNA thereof.
Based on Corman Drosten et al, the subsequent WHO protocols define the short nucleotide sequences which are supposed to specify the genetic fragments used as primers and probes in the SARS-CoV-2 RT-PCR. Until the recent move towards Lateral Flow Devices, alleged case numbers were almost exclusively based upon these tests.
The RT-PCR test was supposed to enable the genetic signature of the virus to be identified in communities around the world. The scientists who criticised the Cormen Drosten paper stated:
[Primers and probes] must be specific to the target-gene you want to amplify..for virus diagnostics at least 3 primer pairs must detect 3 viral genes (preferably as far apart as possible in the viral genome) … Although the Corman-Drosten paper describes 3 primers, these primers only cover roughly half of the virus' genome … Therefore, even if we obtain three positive signals..in a sample, this does not prove the presence of a virus.
This concept of specificity is not shared by the World Health Organisation. The WHO's test guidelines. for SARS-CoV-2 state:
An optimal diagnosis consists of a NAAT [nucleic acid amplification test ] with at least two genome-independent targets of the SARS-CoV-2; however, in areas where transmission is widespread, a simple single-target algorithm can be used … One or more negative results do not necessarily rule out the SARS-CoV-2 infection.
When a team of Moroccan researchers investigated the epidemiology of Moroccan cases of SARS-CoV-2 they found that just 9% tested positive for three genes, 18% were positive for two and 73% percent for just one. Although, reliant upon the WHO protocols, an unknown number may have been positive for none.
The WHO do not require the detection of three or even two viral genes, one is fine. In fact a negative result is still considered a possible indicator of SARS-CoV-2 infection. The repeating of tests is encouraged, presumably until a positive test is returned.
Given that Karry Mullis, the inventor of the PCR test, stated that his technology could "find almost anything in anybody," and that "it doesn't tell you that you are sick," repeated testing is likely to provide a positive result eventually. The UK government's COVID-19 case numbers are actually their claimed number of positive tests. Their testing regime is adapted from the WHO protocols and its guidelines. This alone provides sufficient scientific doubt to question if these numbers are plausible. It is not the only reason.
BLAST It!
When the researchers from the Spanish medical journal D-Salud ran the WHO's specified nucleotide sequences through the Basic Local Alignment Search Tool (BLAST), which allows a comparison with published nucleotide sequences stored by the U.S. National Institutes of Health (NIH) genetic database (called GenBank), they found the WHO protocols matched numerous microbial sequences and genetic fragments of human chromosomes.
For example, a BLAST search for the vital RdRp SARS-CoV-2 sequence revealed ninety-nine human chromosome with a 100% sequence identity match and one hundred matched microbes, with a 100% sequence identity match. The Orf1ab (E gene) returned ninety results with a 100% sequence identity match to human chromosomes. A microbial search of the target for the SARS-CoV-2 E gene found ninety-two microbes with a 100% match.
The so called unique genetic markers for SARS-CoV-2, recorded in the WHO protocols, are not unique at all; literally finding anything in anybody. This does not mean that SARS-CoV-2 is absent but it casts considerable doubt on the process. Indeed the whole concept of viruses can be questioned.
Terrain Theory
Just as Koch, Pasteur and Lister can be seen as the formative minds behind germ theory so Claude Bernard and Antoine Bechamp proposed an entirely different model of disease called terrain theory. Rather than seeing germs (bacteria, fungi, archaea & virus - or the microbiota) as external threats to be repelled, Bechamp and Bernard considered them to be part of human physiology.
Terrain theory is fiercely ridiculed by scientific orthodoxy and the allopathic medical establishment. With a global pharmaceutical and healthcare industry worth trillions of dollars, based upon the idea that viruses and other microbiota attack people, perhaps that isn't surprising. However modern mainstream science appears to be unavoidably adding some weight to terrain theory.
Research by the scientists who participated in the National Institute of Health Human Microbiome Project (HMP) discovered that only 43% of our bodies consist of human cells. The other 57% are microbiota, more commonly called germs (not to be confused with germ cells). Researchers from the HMP stated:
The microorganisms that live inside and on humans (known as the microbiota) are estimated to outnumber human somatic and germ cells by a factor of ten. Together, the genomes of these microbial symbionts (collectively defined as the microbiome) provide traits that humans did not need to evolve on their own. If humans are thought of as a composite of microbial and human cells, the human genetic landscape as an aggregate of the genes in the human genome and the microbiome, and human metabolic features as a blend of human and microbial traits, then the picture that emerges is one of a human supra-organism.
Germs are very much part of our physiology, just as Bechamp and Bernard contended. In fact, they appear to be the dominant part.
If more than half of our physiology is comprised of germs it is difficult to understand how they can be considered simply as invading threats. Within our virome (which is part of our microbiome), viruses in particular appear to number in the trillions.
Given that the field of virology has apparently studied less than 1% of these viruses it seems remarkable that the few viruses that necessitate drug treatments just happen to be within this small minority of known pathogens. Presumably the other 99% are all benign.
Cytopathic Effect
Bechamp and Bernard thought that microbes (germs) were pleomorphic (capable of physically adapting - morphing - to suit their environment). They considered them to be a vital component of physiology and not external threats.
They hypothesised that their morphology was dependent upon the terrain of the human body. Their form and function was seen as response to the condition of the human host. Where that terrain was unbalanced (toxiotic), perhaps due to poor diet or environmental poisons, germs (including viruses - although they didn't know of them at the time) could start the catabolic (disintegration) processes of cells. Modern virologists call this the cytopathic effect.
Thus good health was seen as being much more about prevention than cure. Good nutrition, a clean water supply, a pollution free environment, general fitness, psychological and spiritual health were considered more important in combating disease than destroying parasitic microorganisms. While germs (such as viruses) were still seen to exacerbate and contribute towards cytopathic effects (cell death) it was the toxiotic state of the terrain (conditions), not the germ, that instigated this potentially fatal cascade.
Further evidence seemingly supporting terrain theory can be seen in the public health records. Vaccines exemplify the allopathic model as they are said to be a barrier against invading viruses. Yet a 1977 study by the Boston Department of Sociology found that more than 90% of the huge improvements in U.S public health occurred prior to 1950 — before the widespread use of vaccines.
Improvements in sanitation, water security, diet, income and access to services, were found to be by far the most significant factors. The study estimated that as little as 1% to 3.5% of the improvements could be directly attributed to allopathic medical interventions, of which vaccination were but one facet.
A 2000 study by John Hopkins University and the Center for Disease Control (CDC) corroborated these findings:
… vaccination does not account for the impressive declines in mortality seen in the first half of the century … nearly 90% of the decline in infectious disease mortality among US children occurred before 1940, when few antibiotics or vaccines were available.
Huge reductions in disease and mortality occurred during this period that had little to do with allopathic medical advances. Terrain theorists suggest that inequality and deprivation breed disease, not because pathogens fester in slums but because people fester in slums.
Dr Rudolph Virchow, the renowned father of modern pathology was strongly opposed to the germ theory of Koch, Pasteur and Lister. He saw disease as a political issue, with its roots firmly in inequality of opportunity and resultant poverty. He said "Medicine is a social science, and politics is nothing else but medicine on a large scale.” Perhaps it isn't only pharmaceutical corporations and healthcare providers who have a vested interest in the total rejection of terrain theory.
It is equally true to point out, though, that those who believe in the importance of the terrain often attack germ theory. Perhaps this adversarial approach fails to appreciate the relative strengths and weaknesses in both disease models. While the truth is absolute, we don't have much chance of discovering it with ego and the denial of evidence blocking the path.
Is COVID-19 a Hoax?
To suspect that COVID-19 is a "hoax" is not to dismiss the very real impact the events of the past twelve months have had on families across the UK. Clearly many thousands have died and those deaths have been attributed to a respiratory disease called COVID-19.
No one who criticises the evidence base for COVID-19 is denying that, and they are certainly not dismissing the pain felt by the bereaved.
Until the late 19th century people quite regularly died of "consumption." It wasn't until the development of germ theory that it was realised that this was Tuberculosis.
Koch, Pasteur and Lister weren't disrespecting the lives lost to consumption by questioning the nature of disease. They were examining the medical and scientific evidence and forming scientific theories based upon those observations.
Herein lies the problem for anyone who questions the official COVID-19 narrative. We are living in a time where rational inquiry itself is under attack. It seems that to question the validity of COVID-19 is verboten. Yet clearly, there are justifiable reasons for doing so.
The fake moral outrage of the mainstream media, fact checkers and professional "debunkers," is a defence mechanism and a propaganda technique. It isn't designed to combat the claims of a relatively small group of sceptics; its purpose seems to be to stop the much larger group of somewhat sceptical people looking at the evidence.
You can read more of Iain's work at In This Together.
