
There exists a raft of subjects upon which the views of clerics and medics may be assumed to diverge, but a most powerful magnet of convergence for all should be the principle of doing no harm. The examination of such apparent unity leads into a treacherous mire, especially where human genitalia is concerned. Stones overturned have exposed inconsistency and double-standards, a good deal of looking the other way and abject failure by so-called leaders to present any challenge to an extremely pernicious ideology.
The surgical removal or modification of human genitalia is a somewhat gruesome and most controversial subject. It is also one which illustrates the many and varied contradictions which exist within the espoused positions and practices of the medical professions and the religious faiths in the United Kingdom. We are told, insistently and incessantly, that gender affirmation surgery (GAS) is good, and we are told, less so these days, that female genital mutilation (FGM) is bad. As for the debate surrounding male circumcision, it is barely audible. However, whilst the results of each of these practices—in that genitalia is removed or modified—are identical, the messaging surrounding them could hardly be more different.
The approved method for explaining such differences is to consider the factors of consent, age, harm and medical necessity. It is put forward that those undergoing gender affirmation surgery have chosen to do so, in an informed fashion, which means that they consent to the harm to be inflicted by the surgeon. As to age, the bar for GAS is set at 17 in England, 16 in Scotland, 18 in Wales and 18 in Northern Ireland, for now. It is important to note that so-called ‘puberty blockers’—drugs which affect normal physical changes in the bodies of developing children—are available to minors from the NHS. The NHS has this to say:
Little is known about the long-term side effects of hormone or puberty blockers in children with gender dysphoria’ and it’s also not known whether hormone blockers affect the development of the teenage brain or children's bones.
But despite this, the NHS prescribes them anyway. It is the creation and labelling of gender dysphoria as a clinical illness which enables the construction of any argument in favour of medical necessity.
In a way, age and consent may be dealt with together. Whilst it is, of course, fair to say that FGM is almost exclusively conducted when girls are young, it should be pointed out that male circumcision is almost exclusively conducted at a young age in boys. There may not be a close comparison to make in terms of outcomes or pain, but it is absolutely true that—in most cases—neither is performed with the consent of the subject, as they are not old enough to give it. If it is possible to carry out male circumcision before adulthood, when there exists no medical necessity, the case against FGM is found wanting. Another issue that crops up regularly in this discussion is that of Gillick competence; a most dangerous piece of case law. The situation most often used to explain Gillick competence posits that a child, if deemed competent, may consent to an immunisation without parental consent; even if the parents do not wish for the child to have the immunisation. You are likely to guess the next part. If the child is competent, and does not consent to the immunisation, but the parent wishes the child to be immunised, the parent’s wishes take precedence. With hormone treatment, if a child is deemed competent, he or she may not be denied access to medication. The suggestion that a child could have got to this point with no external influence is patently absurd.
If it is the creation of so-called medical necessity via gender dysphoria that has given rise to the possibility of state-funded genital surgery, then what—if any—are the medical reasons for the practices of FGM and male circumcision? The BBC says:
The most frequently cited reasons for carrying out FGM are social acceptance, religion, misconceptions about hygiene, a means of preserving a girl or woman's virginity, making the woman "marriageable" and enhancing male sexual pleasure.
The NHS explains:
Female genital mutilation (FGM) is a procedure where the female genitals are deliberately cut, injured, altered or removed for non-medical reasons.
This could just as readily describe gender affirmation surgery. However, it clarifies the position by noting that ‘FGM is illegal in the UK and is child abuse’. As to male circumcision in boys, the Health Service says, ‘It's rare for circumcision to be recommended for medical reasons in boys’, thus skating over the much more common cultural or religious reasons. They do go on to refer to the risks associated with the procedure—which are, of course, described as ‘small’.
Even if the origins of FGM and male circumcision are lost in the sands of time, there are still many people today that believe there are compelling reasons for both, which is exactly why they persist. Falling upon a cast-iron means of deciding how to distinguish between them, in terms of social acceptability, is extremely difficult. Assuming each practice is carried out in good faith (which may be an assumption too far for many), the way to explore the difference may be to examine what are referred to as ‘known health benefits’. Around the turn of the last century, Dr Peter Remondino was one of the great cheerleaders for male circumcision and attributed very many health benefits to it; many more than the NHS, at any rate. It is interesting to note that Remondino did also believe the practice would make black men less likely to rape white women and, thus, advocated for ‘the wholesale circumcision of the Negro race as an efficient remedy in preventing the predisposition’. Dr Remondino finds himself at one end of the spectrum, and there are acknowledged risks in male circumcision, but these would appear to be very heavily outweighed by those associated with FGM. In a thoughtful piece for the Guardian, some years ago, Adam Wagner cites the joint statement from the United Nations (UN) and other agencies in 2008, in which FGM is referred to as having ‘no known health benefits’. This would seem to form the crux of the matter, and this point will be returned to.
Gender dysphoria is described by the NHS as ‘a term that describes a sense of unease that a person may have because of a mismatch between their biological sex and their gender identity.’ This hardly reads like the basis for life-altering surgery on the grounds of medical necessity. They go on to explain that ‘Gender dysphoria is not a mental illness, but some people may develop mental health problems because of gender dysphoria.’ However, medical literature on the subject is almost exclusively the preserve of the discipline of psychiatry and, of course, all the ‘signs’ listed by the NHS (shown below) are mental and not physical. Drawing the conclusion that gender dysphoria may lead to mental illness with no allusion to the possibility of things happening the other way suggests an abandonment of the scientific method, at least. Indeed, to go on to suggest that the solution to a problem with exclusively mental symptoms is the physical altering of the human form raises significant questions of medical ethics.
Questionable though the condition of gender dysphoria may appear to be, there is no doubt that the attention given to it suggests there has been an exponential rise in recent years. The NHS website declares that ‘there has been a huge increase in the number of people seeking a referral to a gender dysphoria clinic’. Statistics, as always, are near impossible to draw any firm conclusions from, but those on the transgender spectrum form an incredibly small minority of society. Black’s Medical Dictionary reckons on about 0.0015% of the population having gender dysphoria, whereas the results of a survey published in the Journal of Adolescent Health indicated as many as 1.2% of respondents in New Zealand high schools reported being transgender. Since 1.7% of respondents ‘did not understand the question’, the conclusions should not be taken as copper-bottomed. However, instead of dismissing it entirely, what is worth paying attention to is that all respondents that were emphatically not transgender reported much higher levels of parental neglect, depressive symptoms, suicide attempts and bullying in school. Are we to believe that children with these sad elements to their lives are experiencing this form of rejection due to their equivocation over gender, or that their mental state has led them to consider their existence through the lens of gender? In 2019, a High Court judge ruled in favour of foster parents who had come under the scrutiny of care services at Lancashire County Council after a third of their fostered children had presented with ‘gender identity issues’. What are the odds? The youngest of these children was only four when he began to transition to becoming a girl.
It was not until 1980 that there was deemed sufficient etiological basis for recognising gender dysphoria as a medical condition, and then only by the somewhat controversial publication: the Diagnostic and Statistical Manual of Mental Disorders (third edition) (DSM). British medics take their lead from the International Classification of Diseases (ICD), which took until 1983 to start considering ‘diagnostic categories like ICD-10’s “transsexualism” and “gender identity disorder of children”’. Forty years later, the sun seldom sets on a country not festooned in Pride flags, signalling its capitulation to the voices screeching for ‘trans rights’. It is scarcely likely that the noisy and angst-riddled campaign which accompanies transgenderism has not influenced the minds of young, vulnerable and impressionable people. As Julie Birchill noted in The Spectator, the way to add some zing to your profile as a Hollywood star is to acquire a transgender child. She downplays the very serious psychological ramifications, but concludes:
In the infant days of Hollywood, an actress was fabled to have led a leopard on a leash along Sunset Boulevard. The stars still love to show off their exotic pets. But there’s something really icky about it when the pets are humans.
By contrast, FGM is reckoned to have had a place in society for around two thousand years, and male circumcision many centuries longer. Whether direct or indirect, the links between world religions and these two practices are very strong indeed. So, although describing male circumcision as a form of genital mutilation may seem outlandish, it does fit the definition. It also muddies the waters when it comes to the sanctity of the human form. Somewhat inadvertently, the Christian Medical Fellowship (CMF) strikes at the heart of the inconsistency. On the one hand, it points out ‘that FGM is not a requirement within any religion’, before going on to state that in ‘both Christianity and Islam there is emphasis on the fact that the human body has been created by God, and that we are encouraged to look after the body and not mutilate it in any way.’ In setting out that FGM—specifically—may not be a religious requirement, CMF infers that some forms of mutilation are acceptable as religious requirements, despite the very teachings it cites.
The position held by CMF is, technically, completely contradictory. Nonetheless, the articulation of this argument provides a template that may be thrown over the lines taken by all major religions represented in the United Kingdom today. For this to be the case, such faith groups must be very confident that FGM does, indeed, have no known health benefits and that male circumcision does have some health benefits. A further inference is that this distinction matters more than the belief that the human form should not be mutilated in any way. Otherwise, how to explain that cutting off parts of genitalia is alright for young boys but not alright for young girls? The contrast is so stark, with religious leaders confident to speak out against the practice of FGM. But, as Adam Wagner points out:
Banning male circumcision would have an enormous effect on religious practice. In Judaism, circumcision is one of the most basic requirements of the religion, although it should be noted that Jewish law prohibits circumcision if it would be unsafe for the child.
Religions have their minds made up on FGM and male circumcision, but surgery related to gender and the notion of gender fluidity elicits mostly confusion and equivocation. Reaching for religious texts is the default action in these moments, but this is beset by the problem of interpretation. There is no shortage of transgender advocacy which makes use of scripture. The Religious Action Centre (RAC) for Reform Judaism holds a long piece by Rabbi David Meyer about gender fluidity in the Torah. Meyer also uses the story of God’s creation of man and woman in the Book of Genesis to suggest that it really includes everything between these two extremes. Meyer refers to the six genders that the Jewish legal tradition has identified historically, and he cites passages in the Kabbalah which tell, specifically, of men turning into women and vice versa:
We have opinions that suggest that Jacob’s daughter, Dinah, was conceived with the soul of a man, but through Divine intercession, was transitioned into a woman. Likewise, the kabbalah teaches that Abraham’s son, Isaac, was ensouled as a woman, but born as a man for the purpose of carrying forward the family’s unique covenant with God.
Taking a leaf from the Church of England’s book, as it were, he studiously overlooks the possibility of any surgery to the genitalia having taken place.
In Conservative Judaism, the ground has been shifting rather more noticeably. As written up for the Women’s League for Conservative Judaism, Rabbi Mayer Rabinowitz put forward the view—in 2003—that a public declaration of intent to change gender must be matched by the relevant surgery, and that such surgery was permitted by Jewish law because of the medical necessity to alleviate gender dysphoria. Jane Rosen, who wrote the article, goes on to explain that that position has been overtaken, and she quotes Rabbi Leonard Sharzer as saying ‘Gender is a social construct: how one dresses, talks, behaves, fits into society’. By contrast, some Orthodox Jews have been castigated for rejecting the LGBT doctrine. Orthodox Jewish schools in the UK had their Ofsted (government inspectorate of schools) rating downgraded after refusing to ‘discuss LGBT-related issues with pupils’. The words ‘diversity, equality and inclusion’ have a lot to answer for and, so far, their relentless pursuit only ever ends in the complete absence of all three. Not only that, but subsection 1A of section 403 of the Education Act 1996 is written precisely to avoid such a situation.
The Hindu Council UK and the Buddhist Dhamma Centre are unequivocal in their support of all things LGBT and appealed to the Government to ban conversion therapy in 2018. The report on this appeal, which appeared in The Pink News, said ‘Hindu philosophy recognises the existence of the third gender, which is known as tritīyā-prākriti or “tertiary nature”. This concept encompasses many different kinds of trans and gender-diverse people.’ The Dhamma Center was quoted as saying:
We believe that all people, independent of their sexuality or gender identity, are treasured and valued beings and are a precious part of the Universe.
Mukhannath is the word used by classical Arabic to describe ‘effeminates at the time of the Prophet Muhammad’, according to the Oxford Dictionary of Arabic Literary Terms and Devices, and this has been seized upon to shoehorn transgenderism into Islam. Said to be court performers, due to their ability at singing, mukhannathūn were, or are, men that have taken on the appearance of women, though there does not appear to be any suggestion that this involved any kind of surgical intervention. This is not a subject the Muslim Council of Britain has spent any time discussing in public, though it did come out in support of the Equality Act of 2010.
The Church of England (CofE), still considered England’s state religion—on paper at least—and no stranger to hot water, issued Pastoral Guidance for use in conjunction with the Affirmation of Baptismal Faith in the context of gender transition in 2018. By using phrases like ‘unconditional affirmation of trans people, equally with all people, within the body of Christ’, the Church neatly dodges the question of whether or not such a person has had their genitalia mutilated. Indeed, the guidance goes on to insist special dispensation is given to transgender baptismal candidates. It dictates that:
The minister should be guided by the wishes of the candidate regarding the way in which past experiences may be mentioned or reflected upon, either in the introduction to the service or if the candidate is to share their testimony. If members of their family are to be present, the minister will wish to be sensitive to their pastoral needs.
It is the institution of marriage itself which casts light on the absurdity of the many positions held by the Church of England. At the time of writing, it is not possible for a same-sex couple to be married in church, though they may receive a blessing. It is possible for someone of another faith to be married in a church. It is possible for people of absolutely no faith whatsoever to be married in a church. And, wait for it, possible that ‘a man or woman who has been issued with a gender recognition certificate may marry someone of the opposite sex in a Church of England church’, decided by the General Synod in 2017. So, unless they are very obviously a couple of the same sex, get ‘em in and pile ‘em high. Why? Assuming monthly attendance in church, the value of a congregant that tips £10 into the plate each time is £120 per annum. A wedding pulls in around £600, so who cares if you never see them again? When playing this version of Twister, is it any wonder that the CofE is in a muddle over transgenderism?
In sticking, doggedly, to the line that “The Church of England welcomes and encourages the unconditional affirmation of trans people, equally with all people, within the body of Christ, and rejoices in the diversity of that body into which all Christians have been baptized by one Spirit,”, any mutilation of genitalia may be ignored. How this fits in with the Church’s much-vaunted exercises in the PR of safeguarding is not clear. What appears to be more clear is that the Church would prefer to slope shoulders when it comes to passing judgement on the industry which has given rise to the phenomenon of transitioning from one gender to another. For an industry it is, and one that has more questions asked of it than it will answer.
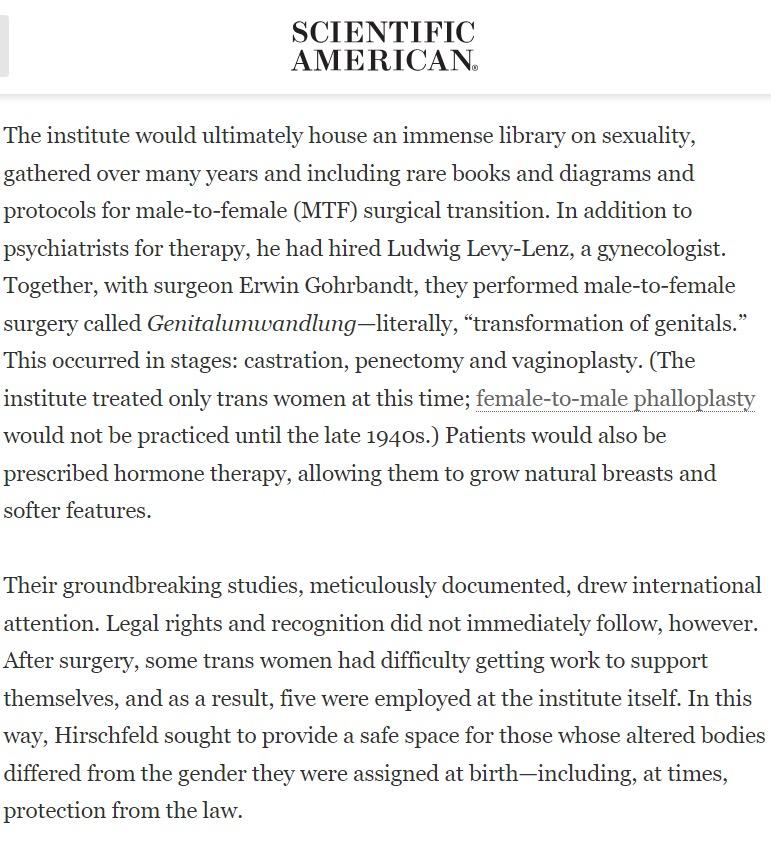
In Berlin in the early years of the twentieth century, a doctor named Magnus Hirschfeld established and ran the Institute for Sexual Research. Hirschfeld, a Jew and a homosexual, developed the concept of a ‘sexual intermediary’ and spent years assisting his clients to live as though of the opposite sex. With a gynaecologist and a surgeon, Hirschfeld pioneered a form of genital mutilation called Genitalumwandlung, which meant ‘transformation of genitals’. The Institute had a vast library on sexuality, and it is now little known that its contents was the first to go up in flames during the Nazi book burning purge of 1933. By the mid-twentieth century, the baton had been grasped by Alfred Kinsey, who put forward that ‘sexuality is on a continuum’ and had conducted a large number of reprehensible experiments on children until he was more or less taken down by Judith Reisman. Kinsey believed that children are ‘sexual from birth’ and even used babies as subjects. Remarkably, the Kinsey Institute still operates out of Indiana University.
The works of those such as Hirschfeld and Kinsey had a profound effect at the time and it should be considered that this effect is still being felt now. The subject matter which has been included in the works of these two men, and others besides, has blurred many lines that should have remained sharp. Just because it may be harmless to dress up as a member of the opposite sex, it does not follow that having body parts removed, or sexualising young children, is also harmless. Clearly, it is not. The question to be asked here is why has medicine and religion done nothing to stop such harm? At this point, the oft-quoted clause from the Hippocratic Oath is tossed out: ‘First, do no harm’. There are several problems with this, not least that this quote has never been a part of the Hippocratic Oath. The original Latin, ‘primum non nocere’, is pretty unlikely to have been written by Hippocrates at all; he was Greek. Just as the Church of England’s goal posts move every time a volley is sent flying, so the oath sworn by British medics has changed considerably over the years. Nowadays, the majority of doctors swear The Physician’s Pledge, last amended by the World Medical Association’s Declaration of Geneva in 2017. It is reprinted below. The construct of doing no harm has been replaced by the altogether more malleable phrase ‘The health and well-being of my patient will be my first consideration’.
In not pledging to do no harm, members of the medical profession have a much freer rein that might be imagined. With regard to gender surgery, The Royal College of Surgeons directs in its Professional Standards:
Ensure that surgery associated with gender reassignment is only undertaken following a referral from a psychiatrist experienced in that field and with a second opinion from an independent psychiatrist also with experience in that field.
Despite the multiple insistences that gender dysphoria is not a mental illness (ICD-11 has moved what it calls ‘gender incongruence’ from the ‘“Mental and behavioural disorders” chapter and into the new “Conditions related to sexual health” chapter’), it looks very much as though it is classed as one for the purposes of any related surgery. Given the many facets to the public debate on sex and gender, it seems a glaring oversight that one of them is not the enabling of such surgery by the surgeons themselves. Just because it is possible to reinvent someone’s genitalia does not mean it should be done; which is why the comparisons with FGM and male circumcision are legitimate. As the General Medical Council notes:
Cosmetic interventions can have a significant impact on the health and wellbeing of patients. There have been particular concerns about patient safety and whether the sector operates in an ethical manner.
The contradictions and inconsistencies presented by the area of any form of genital surgery makes those undergoing it look like victims of a medical profession that has ridden roughshod over the tattered remains of its own ethics. Where gender is concerned, it is irresponsible in the extreme for any faith or religion to celebrate this as a victory for the individual and to fail to examine the circumstances that could have led to it. Safeguarding is cast to the wind by clerics and medics alike, as nobody dare speak out against an ideology that does not bring happiness, no matter how colourful its flags. It is as though the notion of ‘trans rights’ and the fatuous provisions of The Equality Act offer as much protection as these troubled souls will ever need. The spirit of Hirschfeld and Kinsey is now embodied by ghoulish creatures like Yuval Noah Harari, who wrote in his book, Sapiens:
Culture tends to argue that it forbids only that which is unnatural. But from a biological perspective, nothing is unnatural. Whatever is possible is by definition also natural. A truly unnatural behaviour, one that goes against the laws of nature, simply cannot exist, so it would need no prohibition.
This is unspeakable and dangerous bunkum. That the World Economic Forum appears to take its lead from transhumanism enthusiasts such as Harari tells you as much as you need to know.
In choosing to embrace only the social aspect of changing gender and to ignore the trauma, both physical and mental, of surgery to mutilate the genitalia, leaders in faith and medicine are failing catastrophically. Even if Hippocrates has been marginalised, can the medics involved in this really believe they are doing no harm? As to those holding positions of responsibility in religion, what is it that makes them believe that altering the human body like this accords with the teachings in their faiths? These people look as though they are willingly chucking confused, deluded and vulnerable youths—victims of a disruptive transhumanist cult—into an inferno. To return to the longer form of the quote from the UN statement on FGM, it reads as follows:
Female genital mutilation has no known health benefits. On the contrary, it is known to be harmful to girls and women in many ways. First and foremost, it is painful and traumatic. The removal of or damage to healthy, normal genital tissue interferes with the natural functioning of the body and causes several immediate and long-term health consequences.
The sooner people are brave enough to view gender affirmation surgery in the same light, the better.
Main article image: Alisdare Hickson | licence CC BY-SA 2.0

.jpg){kind=link}